
Mr Richard Cobb
Specialist Oral & Maxillofacial Surgeon
- Oral Surgery
- Jaw Surgery
- Facial Surgery
- Skin Surgery
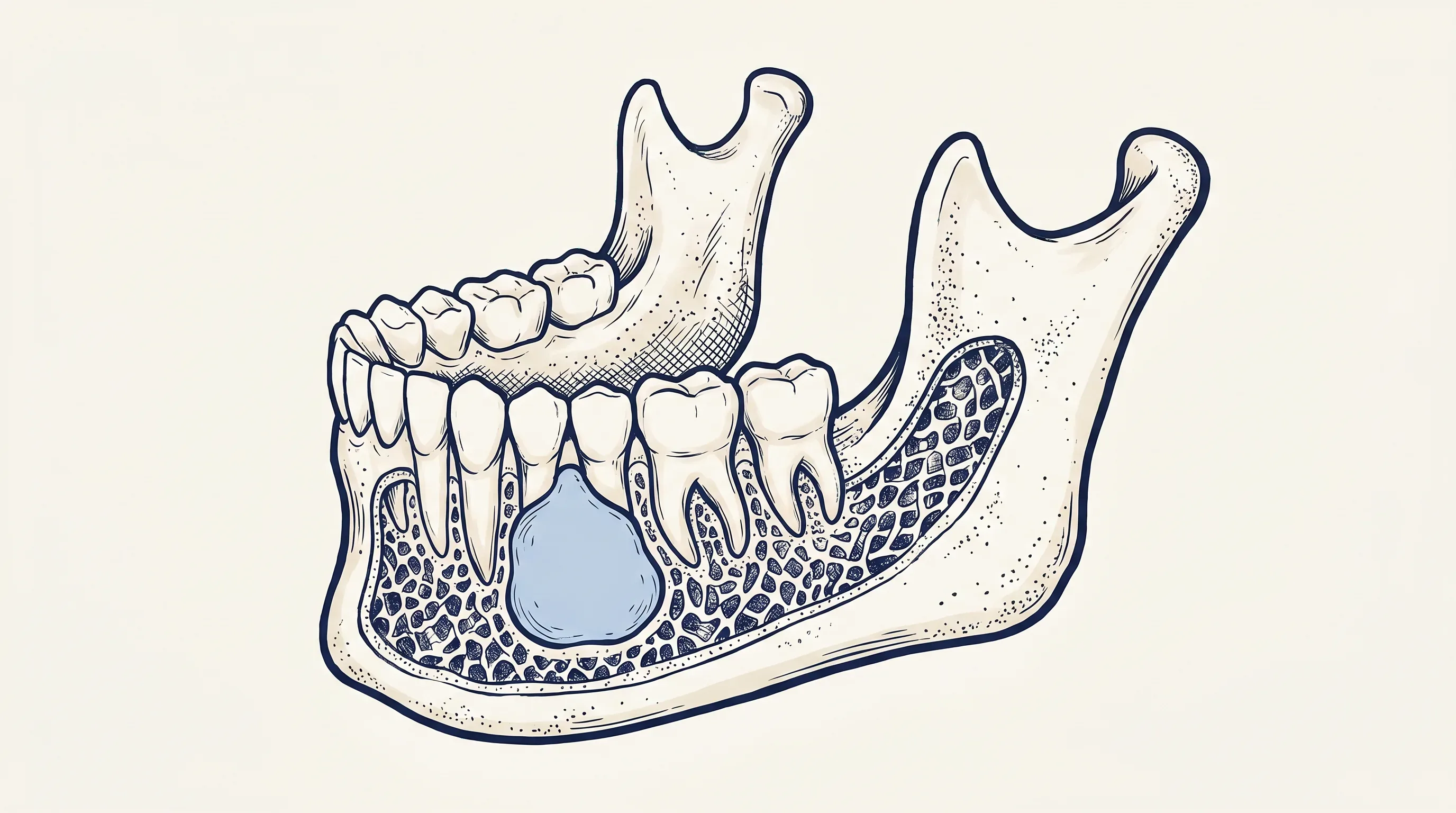
Cysts and tumours of the jaws are often asymptomatic and incidentally found on imaging such as x-rays or CT. These lesions are mostly benign, however some can be quite locally destructive and require careful diagnosis and management. Our surgeons have an emphasis on evidence-based, minimally invasive surgery.

Surgical management of cysts and tumours within the jawbone. Most lesions are benign but some are locally destructive and require careful diagnosis, surgical treatment and long-term surveillance. Our surgeons aim to treat jaw cysts with minimal long-term morbidity.
IS THIS FOR YOU?
Understanding the anatomy
All three surgeons listed below perform this procedure at OMS Specialists. Each carries dual qualifications in medicine and dentistry plus fellowship from the Royal Australasian or English College of Surgeons.
Specialist Oral & Maxillofacial Surgeon

Specialist Oral & Maxillofacial Surgeon

Specialist Oral & Maxillofacial Surgeon
RECOVERY TIMELINE
0–1 day
Day-stay procedure for most cysts. Rest with head elevated, soft diet, ice and prescribed pain medication. Larger resections require hospital admission.
Heavy bleeding, fever over 38°C, or severe swelling not relieved by ice and prescribed medication.
1–14 days
Soft diet continues. Most patients with small cyst enucleation return to desk-based work within 5 to 7 days. Larger resections require longer recovery.
3–12+ months
Bone fills the cyst cavity over several months. For lesions known to recur (e.g. OKC), follow-up imaging and long-term surveillance is scheduled, sometimes for 5 years or more.
| Phase | Duration | What to expect | Red flags |
|---|---|---|---|
| First 24 hours | 0–1 day | Day-stay procedure for most cysts. Rest with head elevated, soft diet, ice and prescribed pain medication. Larger resections require hospital admission. | Heavy bleeding, fever over 38°C, or severe swelling not relieved by ice and prescribed medication. |
| Week 1–2 | 1–14 days | Soft diet continues. Most patients with small cyst enucleation return to desk-based work within 5 to 7 days. Larger resections require longer recovery. | |
| Months 3–12+ | 3–12+ months | Bone fills the cyst cavity over several months. For lesions known to recur (e.g. OKC), follow-up imaging and long-term surveillance is scheduled, sometimes for 5 years or more. |
RISKS & HONESTY
Some lesions, particularly odontogenic keratocysts, have a recurrence rate that requires long-term imaging surveillance. This is discussed at consent and a follow-up plan is agreed.
Cysts and tumours close to the inferior alveolar nerve require careful technique. The risk of altered sensation to the lip and chin depends on lesion size and proximity.
Teeth involved in the cyst or tumour may need to be removed at the same procedure if their support is compromised.
Bleeding and post-operative infection are uncommon and managed with prescribed measures when they occur.
FREQUENTLY ASKED
The great majority of jaw cysts and tumours are benign. Cysts and tumours of the jaws are often asymptomatic and incidentally found on imaging such as x-rays or CT. These lesions are mostly benign, however some can be quite locally destructive and require careful diagnosis and management. Biopsy and histopathology confirm the exact diagnosis and guide the appropriate surgical approach.
Treatment depends on the diagnosis and size of the lesion. Options range from simple enucleation (removing the cyst lining) for small lesions, through marsupialisation (decompressing a large cyst over weeks before definitive removal), to resection with margins for more aggressive lesions. Our surgeons have an emphasis on evidence-based, minimally invasive surgery and aim to treat jaw cysts with minimal long-term morbidity.
Some lesions, particularly odontogenic keratocysts (OKC), have a known recurrence rate and require long-term imaging surveillance, often annually for 5 years or more. The follow-up plan is discussed at consent and reviewed at each appointment.
Teeth that are intimately involved in the cyst or tumour, or whose supporting bone has been destroyed by the lesion, may need to be removed at the same procedure. This is planned and discussed at consultation using imaging.
RELATED PROCEDURES
DIRECT
Online form. Our admin team will respond within one working day.
Request appointmentCLINICIANS
For GPs, dentists and specialists. Secure referral portal with imaging upload.
Refer a patientSPEAK DIRECTLY
Mon to Fri, 8:00am to 5:00pm. Reception will route your call to the right person.
Call (09) 477 0058

